Introduction
Around 2 billion people suffer from latent mycobacterium tuberculosis infection (LTBI) (1). Prevalence of LTBI in health care workers (HCW) in middle and low-income countries ranges between 33 and 79% (2) and in high-income countries it is not higher than 55% (3). Due to professional exposure to tuberculosis patients, health care workers are at increased risk of tuberculosis infection.
LTBI diagnosis has been made for over last hundred years by in vivo method, tuberculin skin test (TST). TST is based on measuring reaction of postponed oversensitivity after a mixture of non-specified mycobacterium antigens (PPD, purified protein derivative) has been injected into the inner surface of the forearm. PPD is used to determine total effect of professional and non-professional exposure to tuberculosis bacillus and the result of reaction is influenced by factors like BCG vaccination (Calmette-Guerin Bacillus) and previous exposure to non-tuberculosis mycobacteria (4,5). Heterogeneity of PPD-solution, subjectivity at reaction reading and different cut-off values for determination of positive TST diminish its specificity. No positive control samples were used in the test and therefore false negative results were possible as consequence of immunosuppressive conditions (6). In countries like Croatia, where BCS vaccination is conducted regularly, TST can give false results.
A new approach to LTBI detection is based on whole human blood ex vivo assays which determine IFN-γ released from T-lymphocytes after their prolonged exposure to M. tuberculosis specific antigens. These antigens distinguish M. tuberculosis from the majority of other mycobacteria (7). This fact specifically contributes to higher specificity of this assay compared to TST. By using IFN-γ releasing assay (IGRA, interferon-gamma release assay) BCG-vaccinated individuals can be excluded, which is not the case with TST. Patients suffering from diabetes mellitus type 1 often have impaired cell immunity and are prone to contagious diseases (8). The aim of this study is to show a LTBI case in a 46 year-old female health care worker (a nurse at the Department for Tuberculosis in young children) suffering from diabetes mellitus type 1. Up to our knowledge, this is the first report of IGRA application in revealing LTBI in an individual who is professionally exposed to mycobacterium tuberculosis and at the same time suffers from type 1 diabetes mellitus.
Case report
A 46 year old female health care worker (a nurse) has been working for 26 years at the Department for Tuberculosis in young children. During the last 20 years she has been suffering from diabetes mellitus type 1. Because of the close contact with tuberculosis patients, she underwent a routine screening for tuberculosis infection.
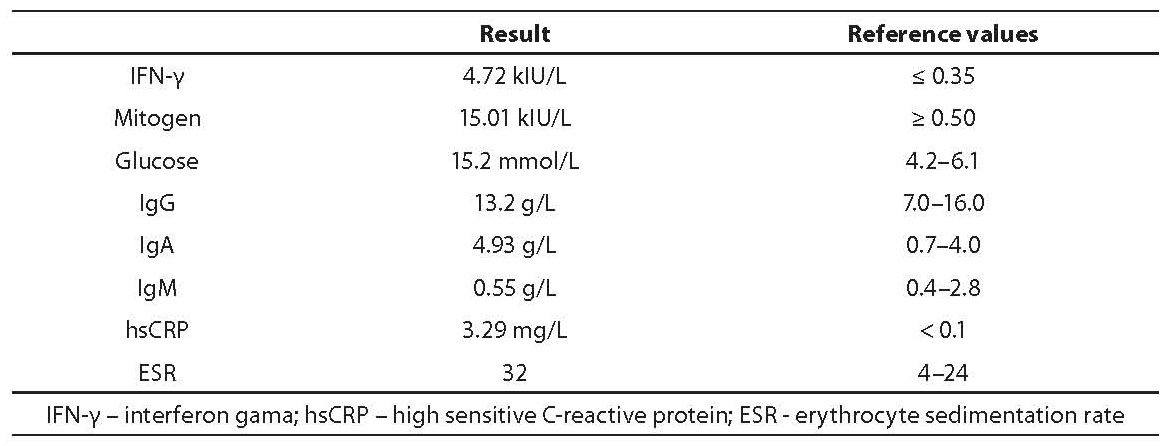
The subject was BCG vaccinated (Bacille Calmette-Guerin) and has a BCG scar. At admission she was not acutely ill, she had normal body temperature, was eupneic and lung auscultation showed normal breathing. TST was negative (induration diameter 6 mm; reading after 72 hours; 2 tuberculin RT-23 units, Statens Serum Institute, Copenhagen, Denmark). Ex vivo IFN-γ test result was positive (≥ 0.35 kIU/L) and positive mitogen control was normal (≥ 0.50 kIU/L). The subject had elevated concentrations of glucose, IgA and hsCRP and elevated erythrocyte sedimentation rate (Table 1).
Table 1. Results of laboratory analyses
Principle of interferon gamma determination after activation with tuberculosis antigens
Venous blood is sampled before TST. Determination procedure is carried out in two phases:
Activation of patient’s whole blood lymphocytes with specific mycobacterium tuberculosis antigens (test tube contains three antigens - ESAT-6, CFP10 and TB7.7). At the same time blood is sampled for positive (test tube with phytohemagglutinin) and negative control (test tube with heparin). All three samples are incubated over night (22 hours) at 37°C, and plasma is thereafter separated and stored at 4°C until analysis (for max 7 days).
IFN-γ concentration determination by ELISA assay with QuantiFERON-TB Gold In Tube (Cellestis Ltd., Victoria, Australia) commercial assay. Test result is displayed as positive if IFN-γ concentration is higher than the cut-off value of ≥ 0.35 kIU/L.
Discission
Only IFN-γ releasing assay (IGRA) indicated the LTBI presence in the nurse who has been for years exposed to tuberculosis patients, while TST result was false negative. Despite diabetes mellitus over many years, active tuberculosis has not developed. From other test results, attention should be drawn to elevated glucose concentration as an indicator of poor diabetes control, and to elevated concentration of inflammatory markers. Elevated IgA concentration can be found in serum in approximately 23% of diabetes mellitus patients, especially if disease has not been treated longer than 10 years (9), which is the case with our female health care worker, or if diabetic nephropathy develops (10). Elevated hsCRP concentration points to latent inflammation which is characteristic for diabetes mellitus patients (11) or to a cardiovascular risk (12).
This case report opens two discussion topics: in vivo and ex vivo test result values for detecting tuberculosis infection in individuals professionally exposed to infectious agent, and relation between tuberculosis infection and diabetes mellitus.
British guidelines for tuberculosis diagnosis and treatment suggest initial screening by TST and positive result confirmation by some of IGRA assays (13). According to US guidelines, the newer IGRA version (QuantiFERON-TB Gold) can completely replace TST assay and it is not necessary to perform both assays simultaneously (14). However, one should bear in mind the diagnostic value of these assays. TST diagnostic value depends on the cut-off value determination that distinguishes positive from negative results (15), and on previous exposure to non-tuberculosis mycobacteria (4). For both assays, population vaccination is very important (16-18). BCG vaccination influences TST test results especially in individuals < 40 years old in countries with low tuberculosis incidence (19). BCG-vaccinated individuals with TST > 11 mm can be considered infected (20). A positive TST result after infection with M.tuberculosis often remains permanently positive (“oncepositive, no longer useful”) (21,22).IFN-γ concentration determination is a better indicator in vaccinated individuals (18) and in individuals longer exposed to M. tuberculosis (23) than TST because it points to acute exposure to specific tuberculosis antigens. Result of the IGRA in people with LTBI showed sensitivity of 90% and specificity of 98% (24). Specificity of IGRA is enhanced by introducing more mycobacterial antigens in the test tube. Test results are simple to interpret when they are comparable. In most studies, concordance between TST and IGRA results could vary between 60-90% (25). In the cases where TST is positive but IGRA is negative, discrepancy could be assigned to prior BCG vaccination (25). Reverse discrepancy (TST negative; IGRA positive) has also been documented in health care workers (26). Agreement of the new generation of IFN tests (Quantiferon-TB Gold, used in the present study) with TST is 79-94 % (27). However, in individuals with impaired cell immunity (patients suffering from malignant diseases, diabetes mellitus, chronic kidney disorder, HIV or on immunosuppressive therapy), results of these assays do not have to be comparable (28). Kobashi et al. showed that immunocompromised patients had negative skin test and positive IGRA test result (23), which is also the case in our study. Therefore, in individuals with impaired immunity, in vivo and ex vivo assays do not have the same diagnostic value as in healthy individuals.
This case report confirms the foregoing statement. It showed false negative skin test result and positive IGRA test result. Such outcome confirmed that, in spite of type 1 diabetes over many years, the IFN-γ releasing reaction toward specific tuberculosis antigens is still preserved. At the same time, by examining cell immunity by IFN-γ determination after phytohemagglutinin-mediated lymphocyte activation, we avoided a possible false negative result. Connection between tuberculosis and diabetes mellitus is a fact known for over 2000 years (29). Already in the 5th century, tuberculosis was described as a complication of diabetes mellitus. Diabetic patients are prone to infections (8) and therefore also to mycobacterium tuberculosis infection. Although there is not sufficient knowledge about the way diabetes impairs the immune system, it seems that this weak immune ability can be attributed to hyperglycemia (30). A study conducted on diabetic mice infected with m. tuberculosis (31) and investigation of the IFN-γ role in individuals suffering from diabetes mellitus also pointed to this causal connection (32). Diabetic mice had inflammatory changes in lungs and at the same time lowered IFN-γ production (31), and individuals with diabetes mellitus were prone to tuberculosis because of IFN-γ deficiency needed for initial growth inhibition of m. tuberculosis (32). Hence we can conclude that, in order to detect low IFN-γ production and consequent susceptibility to active tuberculosis, ex vivo IFN-γ assay should be included in the annual check-up of our subject.