Introduction
Parathyroid hormone (PTH) secretion from parathyroid cells is regulated by action of the calcium on calcium-sensing receptor (1). Vitamin D metabolites and phosphorus have chronic indirect effect on PTH secretion via effects on PTH gene transcription (2) or PTH mRNA stability (3). Measurements of the serum levels of PTH hormone allows for diagnosis and monitoring of several metabolic bone disorders. In last half century many assays for the measurements of PTH levels in the serum or plasma have been developed. It is important to understand characteristics of these assays to be able to make informed diagnostic conclusions from their results.
Secretion and metabolism of parathyroid hormone
The metabolically active parathyroid hormone secreted from parathyroid cells is an 84 aminoacid protein (1–84) PTH. Parathyroid hormone acts on type 1 PTH/PTHrp receptor through interaction of N-terminal portion of the molecule with the receptor. Some degradation of the intact PTH molecule occurs inside the parathyroid cells resulting in secretion of various N-terminally truncated molecules. Some of these fragments have partially preserved N-terminal structure and are called non-(1–84) PTH fragments (4). Others are smaller fragments that lack N-terminal structure (5). The relative amount of the PTH forms secreted is regulated in an acute and chronic manner. Hypocalcaemia causes less intracellular degradation of PTH molecule and more of (1–84) PTH is secreted in relation to other forms. Hypercalcaemia has the opposite effect (6). Chronically, vitamin D deficiency also increases the ratio of (1–84) PTH relative to the fragments. Vitamin D supplementation has the opposite effect.
After secretion, the PTH molecule is quickly degraded in liver (half life of intact PTH is two to four minutes) which releases both, non-(1–84) PTH and C-terminal fragments back into the circulation (4,7). The rapidity of degradation is not affected by level of serum calcium or vitamin D metabolites. Half-life of the remaining fragments of the PTH molecule is five to ten times longer than intact molecule. All molecular forms of the PTH molecule are excreted from the body and degraded by kidneys proportional to the glomerular filtration (7). This is the only known pathway of C-terminal fragment excretion from the body. Consequently, the concentration of the C-terminal fragments exceeds the concentration of intact PTH molecules in circulation.
Accurate and reproducible measurement either of the biologically active or intact parathyroid hormone concentration in serum or plasma is helpful for clinical assessment of bone metabolism. This is particularly difficult to achieve in patients with chronic kidney disease, the population in which abnormalities of bone metabolism are particularly common. As renal function diminishes, C-terminal fragments accumulate in the circulation, continuously altering their ratio to the intact PTH and causing difficulties in assessment of bone metabolism in these patients (8).
PTH assays development
RIA assays
PTH assays which were developed in early 1960s utilized radioimmunoassay (RIA) techniques (9). These are most commonly referred to as the “first generation PTH RIA assays”. There were also a few bioassays but these were used mostly for research purposes. The RIA utilizes radio-labeled peptides in competitive displacement assays. For the PTH measurements, highly purified intact PTH or synthetic PTH fragments were used. The single polyclonal antibody was used and physical means were used to separate bound from free-tracer (charcoal, dextran, etc.). There was a wide variability among the early immunoassays in their ability to differentiate between the normal and hyperparathyroid sera (10,11). The main cause of these variations is immunochemical heterogeneity of circulating PTH (12,13). The PTH immunoassays could be divided into four categories based on major epitopes on the PTH molecule against which the antisera are directed.
1. N-terminal assays: the antisera are directed to N-terminal region of PTH. These assays recognize intact and non-(1–84) PTH fragments.
2. C-terminal assays: The antiserum primarily reacts to the C-terminal region and detects a variety of the C-terminal fragments as well as intact hormone.
3. Midmolecule assays primarily recognize intact molecule and fragments that contained the mid region sequence [44–68].
4. Intact PTH assays: Utilize either a single antiserum against the region where PTH is cleaved [28–48] or two antisera directed to N-terminal and C-terminal regions (sandwich assay).
The actual amount of PTH measured in different clinical situations varied from one assay to another because of different molecular species detected but also depending on the factors such as choice of the tracer and antisera, use of purified or partially purified bovine PTH (1–84) standards and other factors (14). Results of these assays correlated poorly with results of bone histomorphometry in patients with chronic renal disease in some but not all studies (14–16).
Studies of relation between PTH structure and function revealed that PTH function depends on the first 34 aminoacids (12). Hence, N-terminal assays had somewhat better predictive power in assessment of the type of bone disorder in patients with end stage renal patients undergoing dialysis but had low sensitivity and proved to be of limited value (19). C-terminal assays on the other hand detected biologically inert C-terminal fragment which had low clearance rate and little biological activity but accumulated in kidney disease (20).
The next generation of assays utilized well characterized N-terminal and C-terminal monoclonal or polyclonal antibodies, one used as capture antibody bound to solid support and other tagged with isotope ligand and used as signal antibodies. These, second generation PTH IRMA assays are also called “two-site” or “sandwich” intact PTH assays, and provide better clinical correlation than N-terminal and C-terminal RIA assays, and have been the preferred method for PTH detection (Figure 1) (14–16).
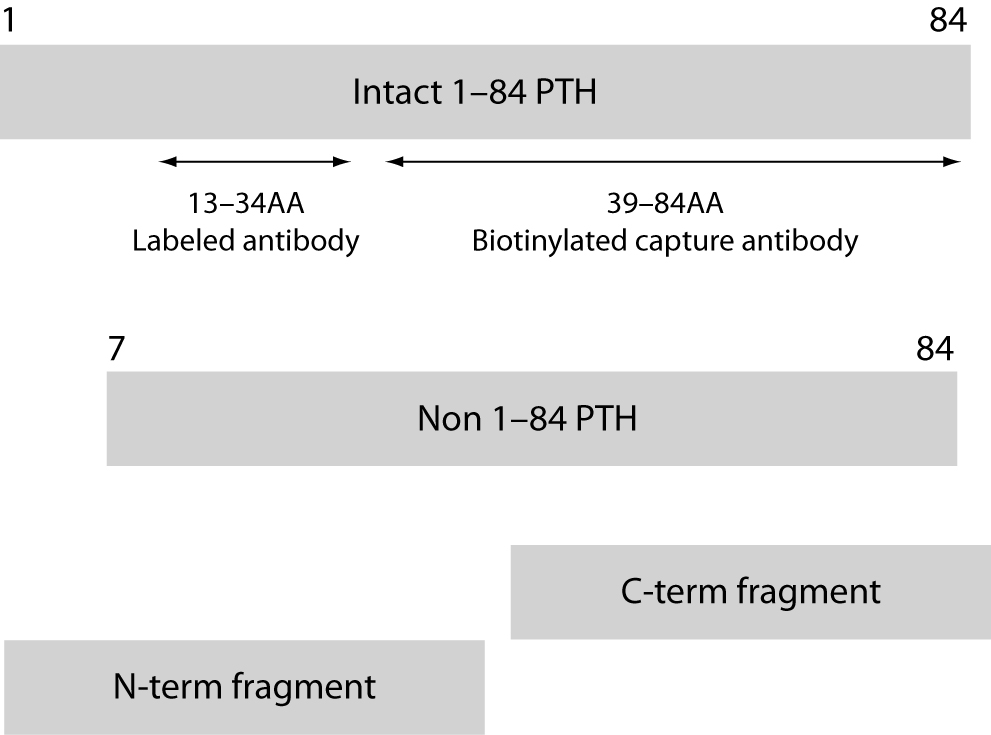
Figure 1. The intact PTH assay uses capture antibody specific for the C-terminal region of the PTH molecule and signal antibody specific for the 13–34 region of the molecule and detects the intact PTH but also the N-terminal truncated long fragments.
The nonisotopic immunometric PTH assays that are developed in late1980s are referred to by various names in literature. We will refer to them as second generation PTH IMA. The original assumption in the development of second generation PTH IRMA and IMA assays was that use of two distinct antibodies will result in detection of the complete, “intact” PTH molecule and allow for accurate measurement of the PTH secretion. Indeed, these assays proved to be far superior to the older RIA assays (14). Reproducibility of the results was much better, even in the patients with end stage renal disease. Studies employing the double tetracycline-labeled bone biopsies showed good correlation of immunometric PTH assay results with the bone histology in patients with different types of renal osteodystrophy (21,22). Results of these studies still guide the interpretation of the PTH levels in patients on dialysis. However, the changes in vitamin D administration to these patients and recent changes in the demographic characteristic of end stage renal patients, both of which have been shown to alter the relationship between the PTH level and bone metabolism, may necessitate reevaluation of bone histology with results of current immunometric PTH assays.
With time it was realized that most of the second generation PTH assays also detect several peptides distinct from the (1–84) PTH, called a non-(1–84) PTH molecular form. Using the high pressure liquid chromatography and/or gel chromatography it is possible to separate many of these peptides and it is realized that truncated segments with partially preserved N-terminal structure, especially (7–84) PTH peptide, are also detected using these assays (23–25). This molecular forms of PTH accumulates in kidney disease and partially accounts for the larger portion of I-PTH in patients with renal failure than in normal subjects and contributes to the major proportion of non-suppressible fraction of I-PTH (25,26). The (7–84) PTH fragment is capable of binding to type 1 PTH/PTHrp receptor but lacks PTH biologic activity, hence competes with and antagonizes PTH action (27–28). This suggests that I-PTH levels overestimate the presence and severity of PTH mediated osseous abnormalities in patients with kidney disease.
In addition, there is a form of (1–84) PTH that is not detected by the second generation PTH IMA tests which use signal antibody specific for epitopes in the 12–18 amino acids region. This form is most likely post-translationally modified in this region, and detection antibodies used in the assays have no specificity for a modified molecule. Such a form of the PTH molecule comprises about 8% of total PTH in healthy individuals and about 15% in renal failure patients (24).
Third generation PTH IMA assays
An ideal assay should possess high precision and accuracy along with a low degree of variation in repeated measurements. Unfortunately both first and second generation assays did not meet the criteria for an ideal assay. Realizing the shortcomings of the second generation PTH IMA assays, efforts were made to develop the next generation of assays that employ the detection antibody that has specificity for the first four aminoacids in the PTH molecule. These assays are called “third generation PTH IMA assays” as well as “biointact PTH assays”. The specificity of these assays was confirmed by their inability to detect synthetic PTH fragments lacking one or more N-terminal aminoacids (29).
These assays are not in routine clinical use presently but several studies have been published comparing performance of the second and third generation PTH IMA assays.
Most of these studies demonstrated excellent correlation of results between second and third generations of PTH IMA assays in healthy individuals, and in those with chronic kidney disease (29–31) resulting in only marginal improvement in clinical performance. The third generation PTH IMA assay results tested over the wide range of plasma PTH concentrations are approximately 40–50% lower than those obtained using the second generation PTH IMA assays (29–32). This indicates that only about half of the immunoreactivity detected by the second generation PTH IMA is attributable to the intact form of PTH while rest is caused by various N-terminally truncated metabolites that retain immunoreactivity. Furthermore, the ratio of intact PTH to these fragments stays relatively constant over the wide variety of PTH levels and renal function.
Clinical comparisons between second and third generation PTH IMA assays
Sensitivity for detection of primary hyperparathyroidism was tested in several studies using the second and third generation PTH IMA assays, and although some studies reached opposite conclusions (33,34), in general it can be said that there is an equivalent diagnostic sensitivity between these two generations of the PTH assays (35). Both generations of assays show excellent sensitivity ranging from 88 to 97% for diagnosis of primary hyperparathyroidism (30,33–35). In addition, in patients with hypercalcemia of malignancy both generations of the assays yield undetectable PTH levels.
Recently, the calcimimetic medications have been introduced into the treatment algorithms for management of secondary hyperparathyroidism in patients with renal insufficiency on dialysis. These medications act through the Ca/Mg receptor and suppress PTH secretion preventing the development of high turnover renal osteodystrophy and tertiary hyperparathyroidism in these patients. Measurement of PTH levels serves as a guide for therapeutic decisions. Comparison of the second and third generation PTH IMA assays showed that both assays could be used for monitoring of therapy with cinacalcet and that this medication does not significantly change the ratio between (1–84) PTH and large, N-terminally truncated PTH fragments (36).
The highest hope for the newest generation of PTH assays was to improve the assessment of the bone turnover in different forms of renal osteodystrophy. However these hopes remain largely unfulfilled. Recent data show that PTH levels obtained by second and third generation PTH IMA assays have very similar predictive power for assessment of bone turnover in patients with end stage renal disease (29,37).
Current shortcomings
The National Kidney Foundation/Kidney-Dialysis Outcome Quality Initiative (K-DOQI) guidelines are used in United States to optimize management of secondary hyperparathyroidism in patients with chronic kidney disease. These guidelines recommend that for stage 5 chronic kidney disease patients (GFR <15 ml/min), PTH level be maintained at 150–300 ng/L (38). This guideline was derived from the series of studies comparing the histomorphometric data from bone biopsies with simultaneous PTH measurements (21,22,39). The PTH levels were determined using the earliest second generation PTH IMA assay, the Allegro assay developed by Nichols Institute Diagnostic Inc. (40). One study examined the question of applicability of this recommendation when assays from different manufacturers are used. Their comparison of 15 commercially available PTH assays, using 47 serum pools from dialysis patients showed a wide range of results. When Allegro intact PTH assay measured values were between 150–300 ng/L, the results with other assays were in 83–323 ng/L range at lower end of the data range and 160–638 ng/L at upper end of the range (41). These findings indicate the need to use assay specific decision limits for patients with chronic kidney disease and/or need for development and application of a correction factor for each assay to make results comparable.
Another study examined the predictive value of PTH measurement for detection of adynamic bone disease and secondary hyperparathyroidism in end stage renal disease patients and found adynamic bone disease in 89.2% of patients with intact PTH ≤ 100 pg/mL while secondary hyperparathyroidism was found in 89.4% of patients whose intact PTH was ≥ 500 pg/mL. However, majority of the patients had intact PTH values between these two levels and in this group low bone turnover was found in 59% of patients while normal or high bone turnover was present in 41% (42). These findings raise concerns about the reliability of the currently available second generation assays.
In an effort to provide a universal management guideline for all CKD patients across the globe, Kidney Disease: Improving Global Outcomes (KDIGO) group released guidelines to manage Chronic Kidney Disease: Bone and Mineral Disorder (43). The working group appropriately addressed the limitations of the available PTH assays and recommended that PTH should be measured, with standardization within clinics and dialysis units in the methods of sample collection, processing, and assay used. More importantly, in contrary to the KDOQI guidelines, KDIGO guidelines determined that using narrow ranges of PTH defining an ‘optimal’ or ‘target’ range was neither possible nor desirable. In conclusion, better tools are necessary for bone metabolism assessment in patients with kidney disease.
Despite these limitations, new information regarding the PTH metabolism and action keeps emerging and the use of the newest PTH assays continues to play an important role in development of this field of investigation. A good example is a study demonstrating association of increased levels of biointact PTH (third generation PTH IMA) with increased mortality in patients on hemodialysis, while total PTH level showed no such association (44).
Insights in PTH physiology and opportunities for further development
The ability of the different assays for PTH to detect different fragments of the intact molecule provided the tools for detailed study of the secretion, metabolism and physiologic actions of the intact PTH molecule and its metabolites. It has been shown that the (7–84) PTH fragment may have biologic activity. When human synthetic (7–84) PTH fragment was administered to rats it caused lowering of serum calcium and when it was co-administered with human (1–84) PTH or human PTH (1–34), it blunted the calcemic response (27, 28, 31, 45). The same studies indicated that this effect is mediated through the receptor distinct from type 1 PTH/PTHrp receptor known as C-PTH receptor which was characterized in 1995 (46). Such an effect is yet to be demonstrated clearly in humans. The ratio of the (1–84) PTH to non (1–84) PTH is actively regulated in humans as demonstrated in the studies of normal healthy volunteers (47,48). It is, therefore, plausible that similar regulation occurs in the patients with chronic renal insufficiency. Measurements of relative amounts of biointact PTH (third generation of PTH IMA) and long C-terminal PTH fragments (value obtained by subtracting the value of biointact PTH from intact PTH value obtained with second generation PTH IMA assay) may offer better insight into bone metabolism in end stage renal disease patients, as shown in the study (32) of 51 patients which found excellent sensitivity (87.5%) for detection of adynamic bone disease.
While we await the development of the ‘perfect’ assay, standardizing the PTH results against a gold standard is a potential option. But the lack of gold standard PTH assay precludes this. As suggested by Souberbielle et al, applying a correction factor to reduce the inter-method variability of PTH measurement is possible but doesn’t provide a permanent solution to the problem (49).
Conclusion
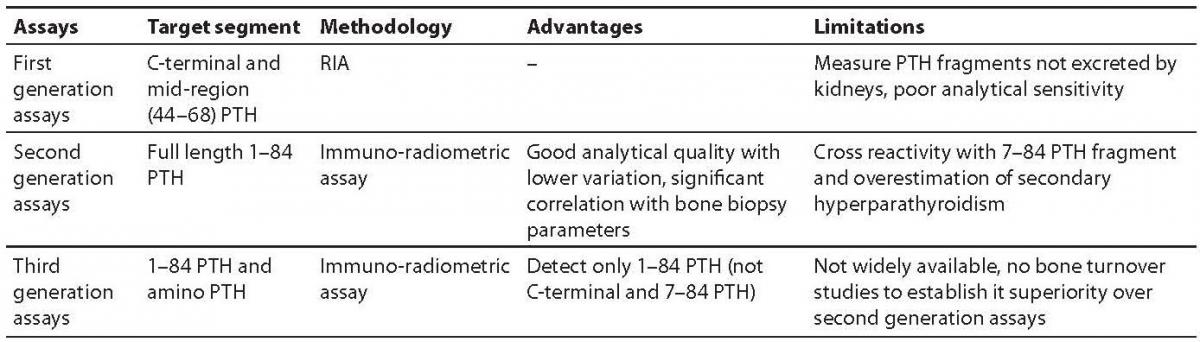
In summary, development of the successive generation of the PTH assay led to the much better understanding of PTH physiology and pathophysiology (Table 1).
Table 1. Characteristics of the various commercially available PTH assays.
Development of the second generation PTH IMA assays in 1980s improved the clinical applicability of the testing, especially in patients with kidney disease. Recognition of the limitations of these assays in detecting of truly intact PTH molecules led to the development of the third generation PTH IMA assays. However, even with third generation assays, the clinical performance of the tests has been improved only marginally. While clinicians strive to provide evidence-based care for these patients, lack of such ideal assays to measure PTH hampers those efforts. Further research in this area is eagerly awaited and necessary to improve our ability to make clinical decisions about treatments of patients with chronic kidney disease.