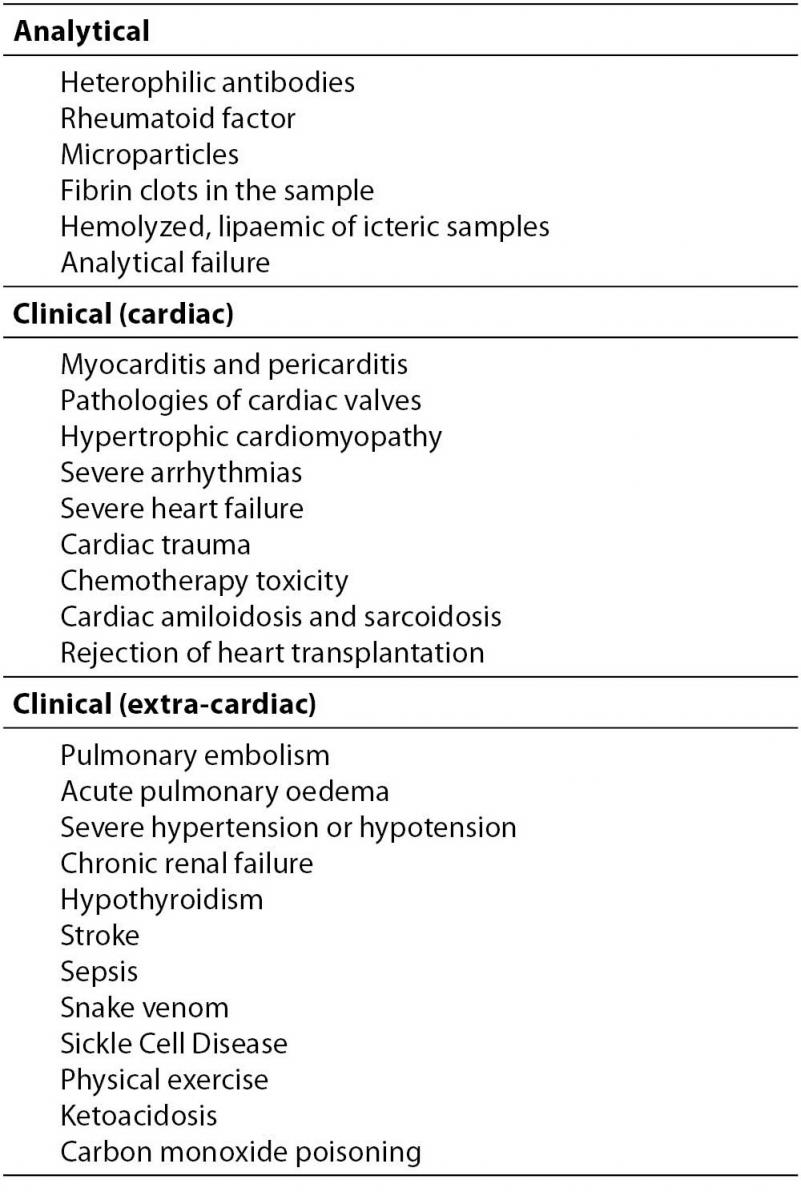
The timely diagnosis of acute coronary syndrome (ACS), in particular myocardial infarction (MI), is still one of the most challenging issues in medicine. Despite the relentless introduction of novel biomarkers of myocardial injury over the past decades, the “Holy Grail” seems to be missing as yet. Although the development and introduction into routine laboratory practice of assays for measuring the cardiospecific troponins (namely Troponin I and T) has dramatically revolutionized the diagnostic approach to the patients with chest pain and suspected ACS, the main drawback of cardiac troponins testing has been represented for years by the relative lack in clinical sensitivity, in that up to 50% of the patients with an ACS had non-diagnostic values on admission (1,2). The recent introduction of methods with improved analytical sensibility (i.e., low limit of detection, LOD), traditionally referred to as “highly sensitivity troponins” (HS-Tns) assays, has substantially contributed to improve the negative predictive value of troponin testing but, contextually, has substantially lowered the clinical specificity of these markers (3). Despite the accurate selection of the normal reference population for calculation of reliable cut-off values (i.e., the 99th percentile limit of the reference value distribution Š99th URLĆ obtained with assays with CV <10% at those levels), there are still several analytical, physiological and pathological conditions where troponin value is measurable in the absence of a clear ischemic myocardial injury (Table 1) (4,5). Physical exercise, especially when strenuous, must be indeed listed among these causes.
Table 1. Main sources of elevations of cardiac troponins in blood.
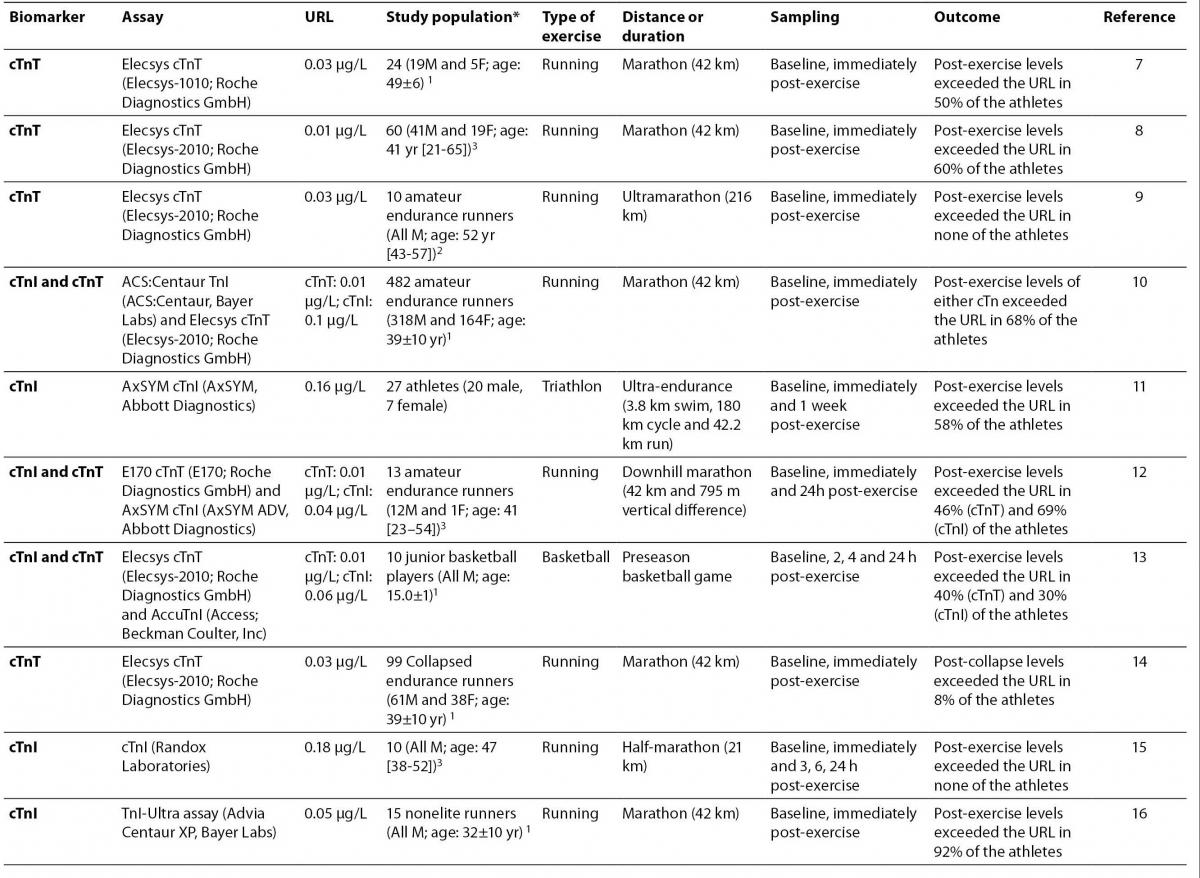
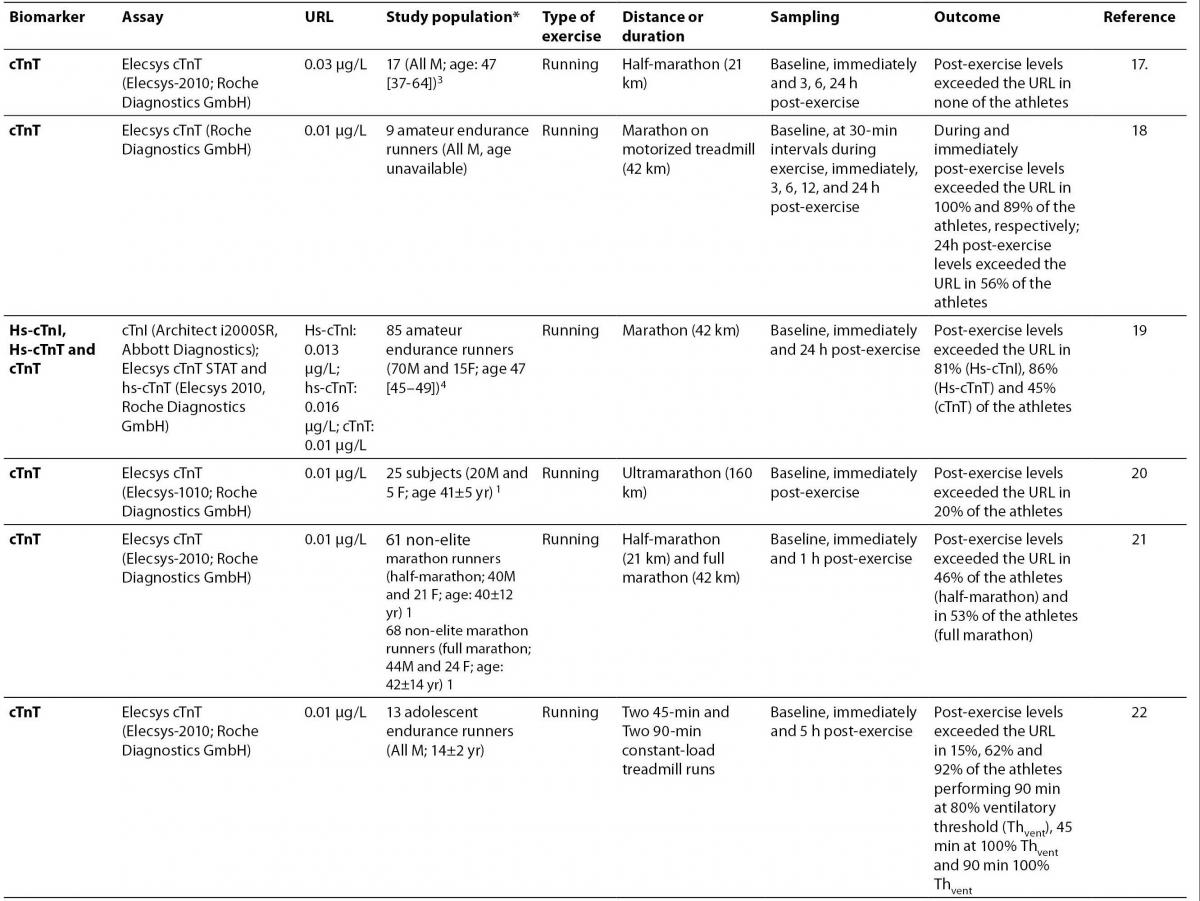
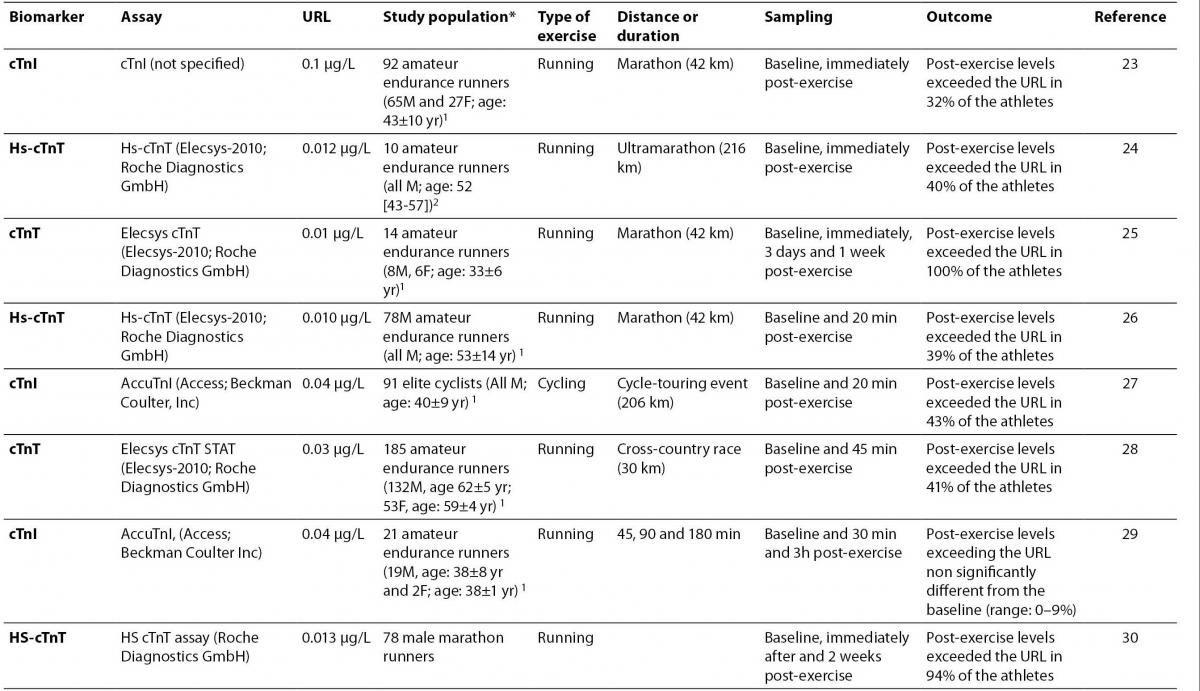
A variety of clinical studies have now clearly demonstrated the existence of an exercise-related increase of HS-Tns (6), with measurable values (i.e., either above the LOD or the 99th URL) being detected in up to 94% of athletes undergoing endurance exercise (Table 2) (7-30). A recent meta-analysis pooling sixteen studies of 939 participants also showed that there were only 6 pre-marathon cTn elevations (0.6%) but as much as 579 post-race elevations (62%) (31). Odds ratio for converting from a normal pre-race to an elevated post-race cTn was 51.8 (95% CI = 16-168; P < 0.001). Interestingly, age and gender were not associated with post-race increases, but publication date and assay sensitivity were indeed associated with cTn elevation. Cardiac TnI was also less commonly elevated versus cardiac TnT, which can be explained with the greater sensibility (i.e., low LOD) of the latter assay. As such, the pooled data of the current scientific literature are consistent with the hypothesis that cTn levels might frequently increase after strenuous endurance exercise.
Table 2. Clinical studies investigating the post-exercise increase of cardiac troponins in endurance sports.
This very frequent occurrence of post-exercise increases of HS-Tns has substantial clinical implications, because diagnostic values in plasma or serum might last for 24 to 36 hours after an acute bulk of physical exercise, and this, in turn if ignored, might dramatically decrease the diagnostic performance of troponin testing, especially in those patients admitted to the emergency department for suspected ACS (32).
Several hypotheses were put forward to explain the biology of troponin increase after physical exercise. Since the current knowledge of myocardial biology has led to definitely rule out that measurable amount of troponins in blood after physical exercise would reflect a clinically threatening myocardial injury, it is now assumed that they would instead mirror an increased membrane permeability and early troponin release (i.e., “leakage”) from the unbound, cytosolic pool, which represents nearly 3-8% of the total cardiac troponin content (33,34). This hypothesis is supported by the fact that the anatomic variations observed in marathon runners only included dilation of the right atrium and right ventricle, reduction of right ventricular ejection fraction, but no morphological changes were observed in the left atrium or ventricle, nor evidence of ischemic injury to any chamber by late gadolinium enhancement could be detected (35). Similar morphological features were observed by Wilson et al., who concluded that biomarkers of cardiac sufferance after prolonged exercise are not associated with either systolic (i.e., stroke volume or ejection fraction) or diastolic (i.e., early diastolic filling [E], late diastolic filling [A], E/A, isovolumic relaxation time, E deceleration time) functional measures (36).
Besides a very low amount of troponin, which is now measurable using most of the novel HS assays and is mainly attributable to cardiac remodelling (i.e., turnover of cardiomyocytes), the stretch-induced release of troponin and its degradation products even in absence of a clear myocardial necrosis has been widely described in several extra-cardiac clinical conditions, such as those listed in table 1. The precise mechanisms of the cellular leakage probably involves a sequence of events, where cardiac ischemia interferes with the normal function of the plasma membrane so that plasma membrane bubbles (also defined “blebs”) develop and gradually grow as a function of both severity and duration of ischemia. Transient or mild cardiac ischemic episodes, such as those occurring during physical exercise, might not be sufficient to produce an irreversible membrane injury, so that the blebs are either reabsorbed or shed into the circulation with their protein content, thus justifying the low (usually < 1.0 µg/L) and short-lasting (typically < 24-36 h) amount of troponin detectable with the new HS assays. Conversely, when re-oxygenation dose not occur timely and cardiac ischemia is thereby prolonged, the blebs at the surface of the plasma membrane tend to collapse rather than be shed into the circulation and the irreversible myocardial injury (i.e., cell necrosis) occurs (34,37). In this instance, the appearance of troponin in plasma is that typical of ACS or MI. As such, the exercise-induced myocardium sufferance can be completely repaired and it might even lead to super-compensation.
A further support for this elegant model has recently been provided with the data of O’Hanlon et al, who demonstrated a non significant relationship between cardiac troponins and measures of cardiac damage. In particular, the increase of troponins and other cardiac biomarkers were unrelated with any detectable myocardial damage (inflammation, oedema, hyperemia, or fibrosis) using current gold standard imaging modalities (i.e., cardiovascular magnetic resonance) (38). It is to mention however that the conclusions from Delayed Gadolinium Enhancement (DGE) studies, in which a lack of enhancement has been argued as evidence that myocardial necrosis does not occur, might be questionable inasmuch as the levels of cardiac troponins detectable in athletes is usually less than that defined as the sensitivity limits for necrosis detectable on DGE following percutaneous coronary intervention or myocarditis.
Cardiac abnormalities may be a major source of morbidity in a small number of endurance and recreational athletes. Neilan et al investigated nonelite participants before and after the 2004 and 2005 Boston Marathons with echocardiography and serum biomarkers (8). Sixty percent of participants had increased cTnT > 99th percentile of normal (> 0.01 ng/mL), whereas 40% had a cTnT level at or above the decision limit for acute myocardial necrosis (≥ 0.03 ng/mL) after the race. Interestingly these troponin increases significantly correlated with post-race diastolic dysfunction, increased pulmonary pressures, and right ventricular dysfunction, and inversely with training mileage. As such, exercise-induced cardiac dysfunction (e.g., right ventricular dysfunction) might be an additional biochemical evidence of cardiac injury after endurance sports, especially in participants with less training.
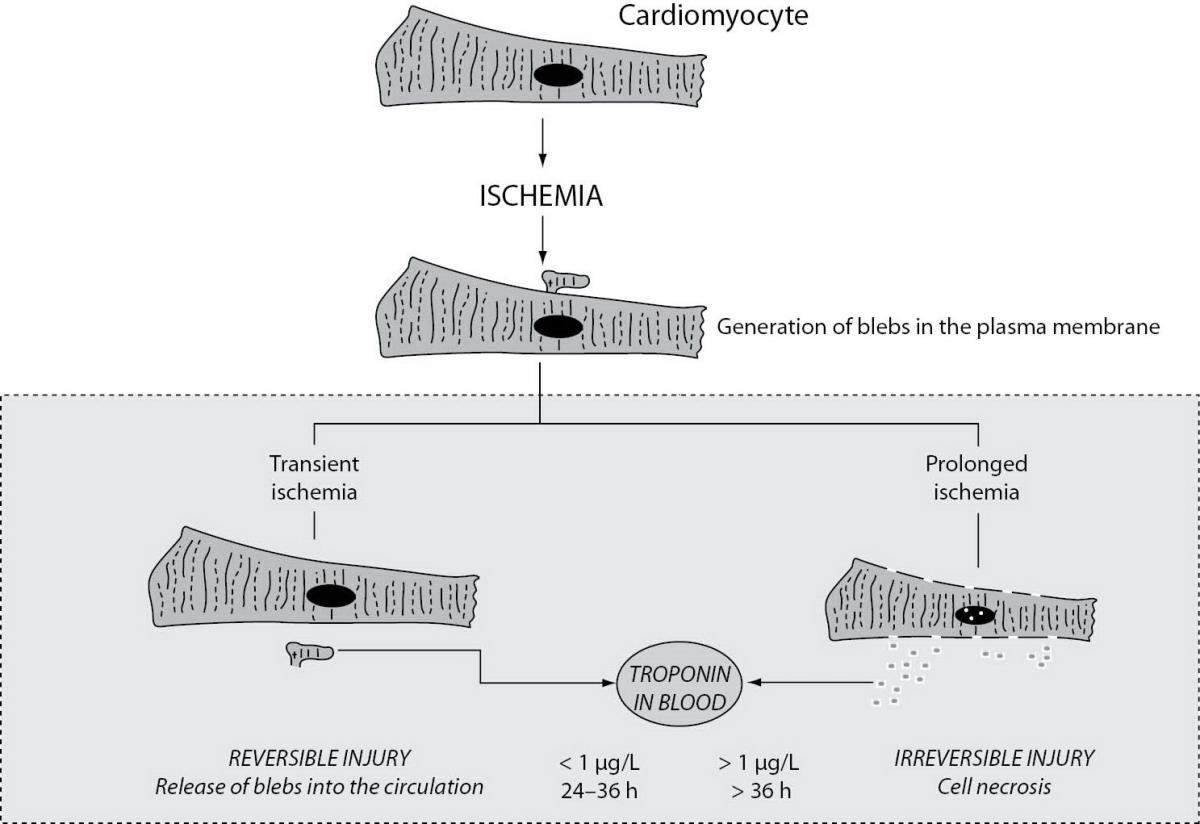
Figure 1. Biological basis underlying the ischemic release of measurable amount of cardiac troponins from cardiomyocites.
Recreational sports encompass activities where the primary purpose is participation, but that also hold the inherent goals of improved physical fitness, fun and social involvement. This kind of physical activity, which includes mostly amateur running and cycling, is typically less stressful, both physically and mentally, for the participants and it is also endorsed by health agencies and organizations such as the American Heart Association (AHA) and the American College of Sports Medicine (ACSM) for the substantial healthcare benefits, both physical and economical (i.e., reductions in the strain on public healthcare costs due to prevention of several pathologies such as cardiovascular disease, cancer and osteoporosis) (39). Nevertheless, the clear demonstration that even moderate amounts of physical exercise can increase the concentration of cardiac biomarkers, especially when measured with the novel HS assays, requires major clinical focus on this issue (i.e., serial measurement of cardiac biomarkers, detailed clinical history-taking, integration with ECG and imaging findings) to prevent misdiagnosis of ACS and/or MI otherwise healthy persons.