Introduction
Migraine is a chronic disorder with complex pathophysiology involving both the metabolism and neuro-vascular mechanism (1). Associations between migraine and vascular disorders such as coronary heart disease and stroke have been reported in previous studies. In addition, an association has been documented between migraine and vascular diseases such as hypertension and subclinical ischemic brain lesions (2).
In recent years, the idea that glucose metabolism throughout the body is coordinated by the brain has gained growing support. Nowadays, there is growing evidence that alterations in the insulin and glucose metabolism may be involved in the pathogenesis of migraine (3). Rainero et al. observed that insulin resistance is more common in patients with migraine (4). Moreover, migraine is a disease with a variety of comorbid disorders, including diabetes mellitus (5). It has long been understood that blood sugar can have an impact on migraine disease; indeed the most frequent triggering factor reported by migraineurs is fasting. Studies suggest that migraine is more likely in susceptible subjects when there is low insulin receptor activation (6-8). Insulin is also thought to influence brain metabolism and cerebral blood flow through insulin receptors, which are found in many parts of the brain (9). Interestingly, it is well known that insulin resistance (IR) is considered to be a risk factor for neurovascular diseases such as hypertension and stroke (10).
In 1976, Robert Turner and Rury Holman developed the concept that fasting plasma insulin and glucose levels were determined, in part, by a hepatic-beta cell feedback loop (11). Many years later, in 1985, David Matthews published an expanded and more comprehensive structural model known as the Homeostasis Assessment Model (HOMA) (12). In 1998, Jonathan Levy published an updated HOMA model (HOMA2) which took account of variations in hepatic and peripheral glucose resistance (13).
On the other hand, the role of free radicals and oxidative stress in neurological disorders has only recently been recognized (14). Oxidative stress is the result of an excessive formation of chemically unstable by-products, called free radicals, within the cell (15). Under normal conditions, the cell is able to destroy the free radicals; however, when excessive free radicals accumulate, these molecules mount an attack against the cell in search of chemical stability (16). It is considered that brain and neural tissue are more susceptible to oxidative damage than other tissues or organs (17). Enhanced oxidative stress is observed in a number of acute and chronic diseases of the central nervous system. Oxidative stress is also believed to play a role in the pathogenesis of migraine (18).
The main aim of this study was to verify whether migraineurs have abnormalities of the glucose and insulin metabolism, at baseline. A secondary aim was to search for a correlation between serum glucose and/or insulin levels and oxidative balance in patients with migraine.
Materials and methods
Subjects
Sixty patients (48 female, 12 male; age 34 (25-43) years) who had presented at the Neurology Outpatient Clinic of Education and Research Hospital were prospectively included in the study. The patients were evaluated and diagnosed by the same neurologist on the basis of The International Classification of Headache Disorders, 2nd edition (19). Forty-six age- and sex-matched healthy controls (37 female, 9 male; age 35 (26-44) years) were enrolled for comparison.The control group consisted of volunteers from the hospital staff who had never had recurrent primary headaches. All the participants belonged to the same ethnic group and had comparable socioeconomic status. The patients with migraine, or subjects in the control group with an unstable medical condition (e.g. cardiovascular, hepatic, renal or endocrine disorder) within the past 2 years; or the ones using any medications – e.g. lipid lowering agents or antioxidant drugs - that could influence the results, were excluded. Patients were headache-free for at least 24 hours. All subjects had full physical examination and were asked to complete a general questionnaire and gave informed consent before the onset of study. The self-limited questionnaires were the gold standard for measuring disease activity and functional capacity in patients. The following data were recorded for each patient: age, sex, age at onset of disease, number of days with headache per month (less than 3 days, more than 3-less than 12 days, more than 12 days), severity of headache (mild, moderate, severe), chronic treatments, alcohol consumption, smoking, family history of cardiovascular disease. Blood pressure was measured manually with a sphygmomanometer. Hypertension was defined as systolic blood pressure of at least 140 mm Hg, diastolic blood pressure of at least 90 mm Hg, otherwise physician diagnosed hypertension. Body mass index was calculated as weight in kilograms divided by height in meters squared.
This study was performed in accordance with the ethical standards set by the Declaration of Helsinki and was approved by the local ethics committee.
Samples
Blood samples were obtained after an overnight fast. Serum samples were then separated from the cells by centrifugation for 10 minutes at a centrifugation force of 3000 x g. Glucose and insulin were measured immediately after sampling. Remaining serum portions were stored at -80 °C and used to analyze Total Oxidant Status (TOS) and Total Antioxidant Status (TAS).
Measurement of the serum glucose, insulin and HOMA –IR index
The levels of fasting glucose were determined by using commercially available assay kits (Abbott Diagnostics, Abbott Park, Illinois, USA) with an autoanalyzer (Architect ®c16000, Abbott Diagnostics, Abbott Park, Illinois, USA). Serum insulin levels were measured using an automated chemiluminescence autoanalyzer (UniCel® DxI 800 Immunoassay System, Beckman Coulter, Krefeld, Germany). The insulin resistance index was calculated on the basis of fasting values for glycaemia and insulinemia, according to the homeostasis model assessment (HOMA): insulin resistance (HOMA-IR) = fasting insulinaemia (mU/mL) × fasting glycaemia (mmol/L)/22.5 (12).
Measurements of the total oxidant and antioxidant statuses of serum
The TAS and TOS of the serum were measured by commercially available kits (Rel Assay® Diagnostics, Gaziantep, Turkey) with an autoanalyzer (Architect ®c16000, Abbott Diagnostics, Abbott Park, Illinois, USA), using novel automated colorimetric measurement methods for both statuses developed by Erel (20,21). In TAS method, which has a precision value lower than 3%, antioxidants in the sample reduce dark blue-green colored 2, 2’-azino-bis (3-ethylbenzthiazoline-6-sulphonic acid) (ABTS) radical to colorless reduced ABTS form. The change of absorbance at 660 nm is related with total antioxidant level of the sample. Using this method, the antioxidative effect of the sample against the potent free radical reactions initiated by the produced hydroxyl radical, is measured. The results are expressed as micromolar trolox equivalent per liter (22,23).
In TOS method, which also has a precision value lower than 3%, oxidants present in the sample oxidize the ferrous ion–chelator complex to ferric ion. The ferric ion makes a colored complex with chromogen in an acidic medium. The color intensity, which can be measured spectrophotometrically, is related to the total amount of oxidant molecules present in the sample. The results are expressed in terms of micromolar hydrogen peroxide equivalent per liter (μmol H2O2 Equiv. /L) (22,23)
Oxidative Stress Index
The percentage ratio of TOS level to TAS level was accepted as oxidative stress index (OSI) (24). The OSI value was calculated according to the following formula: OSI (arbitrary unit) = TOS (micromolar hydrogen peroxide equivalent per liter)/TAS (micromolar trolox equivalent per liter (25).
Statistical analysis
Statistical analyses were carried out using the statistical software version 11.5.1.0 (MedCalc®, Mariakerke, Belgium). In normally distributed groups the results were presented with mean and SD, otherwise with medians and interquartile range. Data on age are presented as median and range. The significance of the differences between groups was determined by Student’s unpaired t-test for normal distributions, and by the Mann–Whitney U-test in abnormal distributions. Pearson correlation coefficient and Spearman correlation coefficient were used to test the strength of any associations between different variables. P values less than 0.05 were considered statistically significant.
Results
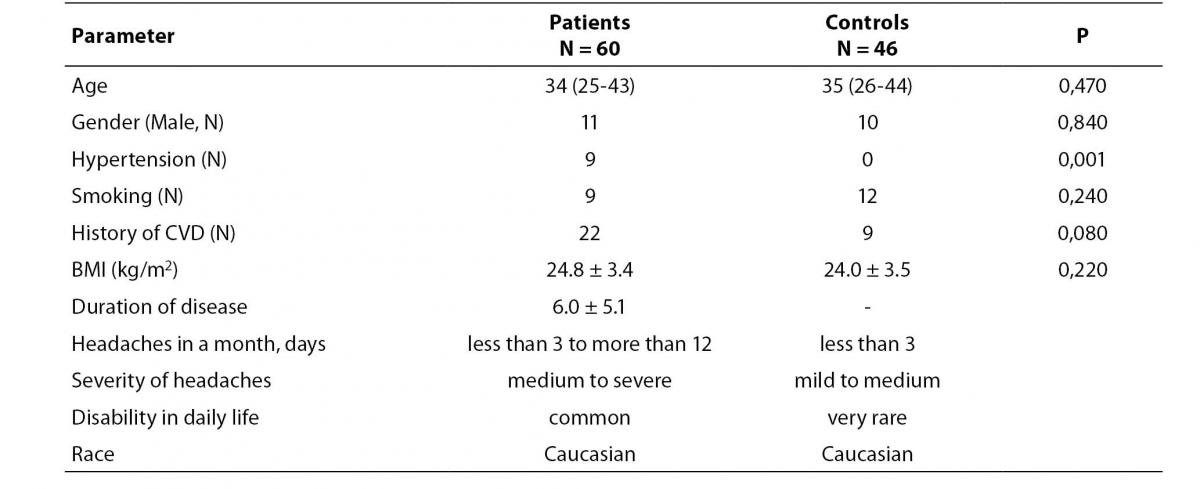
Demographic and clinical data of migraine patients and controls are summarized in Table 1. The female migraineurs (81%) dominated the patient group as expected. Our control group was free of hypertension making the P value significant automatically. The questionnaire gave us detailed information about the duration of disease, number of days with headache attacks in a month, severity of pain and how effective the headache was in the migraineurs’ daily life (Table 1).
Table 1. Demographic and clinical data of migraine patients and controls
Compared to the control group, serum fasting glucose, insulin levels and HOMA-IR index were statistically significantly higher (P < 0.001, P = 0.026, P = 0.038, respectively) in the patient group. We also observed that TOS levels and OSI were significantly higher in migraineurs (P < 0.001 for both), as shown in Table 2. It was interesting to observe that migraineurs having a headache frequency of less than 3 days per month (N = 22) showed a lower HOMA-IR level compared to the ones having a headache frequency of more than 3 days but less than 12 days per month (N = 33) (P = 0.050). Statistical analysis showed a weak positive Pearson correlation between TAS and HOMA-IR in the control group (r = 0.296, P = 0.045); and a weak positive Spearman correlation between BMI and HOMA-IR (r = 0.282, P = 0.030) in the migraine group.
Table 2. Levels of biochemical parameters in patient and control group of subjects

Migraine patients were divided into two subgroups, namely with-aura (MWA) and without-aura (MWOA) migraineurs. We did not observe any significant differences between the subgroups, other than a lower fasting glucose level in aura positive subgroup (P = 0.015) (Table 3).
Table 3. Serum fasting glucose, insulin levels and HOMA-IR index, TAS, TOS and OSI levels of migraineurs with and without aura

Discussion
Chronic oxidative stress may lead to degeneration of neurons and the degenerative diseases. Thus, it has been shown that oxygenated free radicals are able to alter vascular function and to disturb cellular homeostasis (26). On the other hand, elevated extra and intracellular glucose concentrations result in an oxidative stress. Evidence has accumulated suggesting that diabetic patients are under oxidative stress and that complications of diabetes seem to be partially mediated by oxidative stress (27).
The migraineurs in our study had higher basal plasma insulin levels and raised basal plasma glucose values. A higher basal plasma insulin level probably causes the basal plasma glucose to rise until the reduced number of beta cells are stimulated enough to secrete a normal basal insulin level (28). The increased plasma glucose load further stresses the remaining beta cells which then have to operate closer to their maximal capacity in migraineurs (29). Accordingly, McCarty et al. recently reported that five single-nucleotide polymorphisms within the insulin receptor gene showed significant association with migraine (30). In addition, Gruber et al. investigated the insulin and glucose metabolism in migraineurs and showed that hyperinsulinaemia was associated with migraine and, furthermore, was correlated with increased nitric oxide stress (31). The magnitude of the basal plasma insulin gives a measure of the degree of insulin resistance associated with impaired oxidative balance (31). Insulin resistance may also be associated with an intracellular production of free radicals, which in turn could be responsible for a deterioration of insulin action, thus leading to a vicious circle (32). In a recent study, Bourquard et al. provided evidence that factors secreted by activated paraoxonase 2-deficient macrophages - an enzyme with undefined antioxidant properties and protects against atherosclerosis - are capable of altering insulin signaling consistent with that observed in vivo. (33). Indeed, metabolic disturbances and oxidative stress seem to be tightly related, an improved glycemic control being associated with a lowering of the prooxidant status.
We have found higher levels of plasma total oxidant status and higher OSIs in migraine patients compared to the control subjects. Moreover, the migraineurs having a headache frequency of less than 3 days per month in our study showed a lower HOMA-IR level compared to the ones having a headache more than 3 but less than 12 days per month. Similarly, in a recent study, Alp et al. found OSI to be significantly increased, and total-SH and TAS to be decreased in patients with migraine. They also detected significant negative correlations between total-SH levels and the duration of headaches in the patient group (34). Disorders of oxidant-antioxidant balance underlie a number of acute and chronic diseases of the central nervous system including epilepsy and migraine (35). A relationship between glucose concentration and oxidative stress has been shown in cultured cells. Several mechanisms seem to be involved in the development of an oxidative stress in the presence of elevated glucose concentrations, namely glucose autoxidation, protein glycation, advanced glycation end products (AGE) formation. As glycated proteins, AGEs are also able to produce oxygenated free radicals via complex biochemical mechanisms (36-38). In addition, glucose is reduced by the aldose reductase into sorbitol which is oxidized to fructose by the sorbitol dehydrogenase. NADPH is required for the activity of aldose reductase. Therefore, an enhancement of the polyol pathway results in an intracellular depletion of NADPH (39). Antioxidant enzymes such as glutathione reductase which regenerate reduced glutathione need NADPH. Thus, an intracellular depletion of this cofactor, by decreasing the activity of glutathione reductase (TAS component), decreases the intracellular content of reduced glutathione, which constitutes an important factor for the protection towards oxygenated free radical-induced damages (40,41).
Possible sources of oxidative stress in migraine subjects (enhanced HOMA index) include an increased production of radical oxygen species, especially from glycation or lipoxidation processes, and decreased enzymatic or non-enzymatic antioxidant defense system (42-45).
To conclude, our study provides evidence for a possible mechanism linking impaired glucose metabolism and enhanced oxidative stress index in migraineurs.